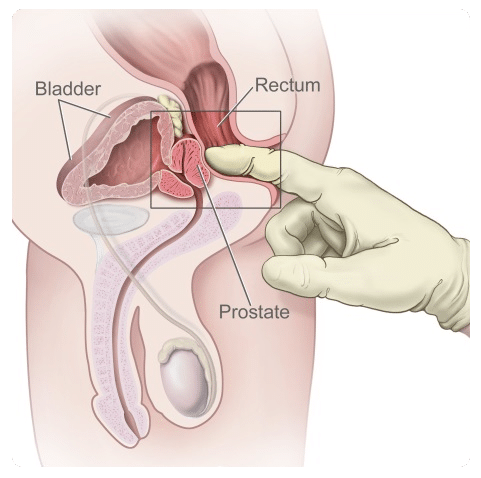
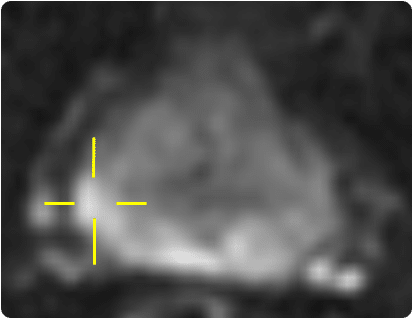
Figure 1

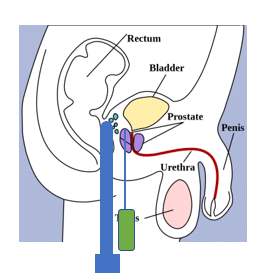
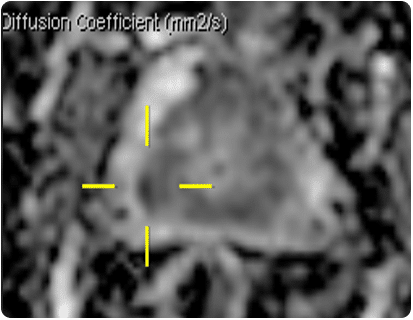
Figure 2
LDR (Low Dose Rate) BRACHYTHERAPY
LDR (Low Dose Rate) BRACHYTHERAPY

ACCURACY & SPEED
These often conflict with each other as the need for accuracy slows the procedure. For LDR brachytherapy a 1.0mm error in a single seed position could result in 20% difference in dose at 10mm from the seed however in reality the error is smaller than this as the multiple seeds will be displaced in different directions. Any displacement from the original planned position will deteriorate the quality of the final plan. A slow procedure can lead to complications with equipment if fluid blood tracks into the needles / applicator. Ideally the time under anaesthetic should be short for both the patients’ benefits and throughput for the hospital. A robotic solution removes intra-operator variability and has potential to be consistently quicker than the manual method.

FLEXIBILITY OF SEED / SOURCE POSITION
This should be fully flexible for optimal dose distribution. Whilst with the current technique the needles can be steered to some extent, approximately 2mm in each direction, this is difficult to achieve and may require multiple attempts before achieving the correct needle (and subsequently seed or source) position. This affects the speed of the procedure and is likely to be linked to patient discomfort following the procedure. A robotic solution with needles designed with greater flexibility for steering will address this. Number of punctures: This may be as many as 30 through the perineum (or rectum in the case of trans-rectal biopsies). It is known that the trans-rectal approach has a raised rate of complications relative to the trans-perineal approach [20] and therefore the trans-perineal approach will be used. However the trans-perineal approach can lead to more frequent mild pain post procedure [20] which has the potential to be limited by reducing the number of puncture holes needed in the robotic system to only 1-4 and steering the needle to the required location from here.

QUALITY OF BIOPSY CORES
The current technique can lead to poor quality cores taken by the clinician if the needle is not well positioned or if the biopsy gun is not fired correctly, which leads to increased procedure time. For the pathologists, analysis of prostate cores is more complex if the sample is poor, and in some circumstances, a core may be taken but there is insufficient prostate tissue for analysis.